- 如有疑问,请联系电邮
- customer@ihealth66.com


USNEWS:不喜欢做结肠镜检查的人还有6种新选择!

USNEWS:为什么孩子吃饭不好?生理还是心理问题?
2019年4月29日
USNEWS:生活中你不应该忽视的10个看似无辜的身体改变!
2019年5月5日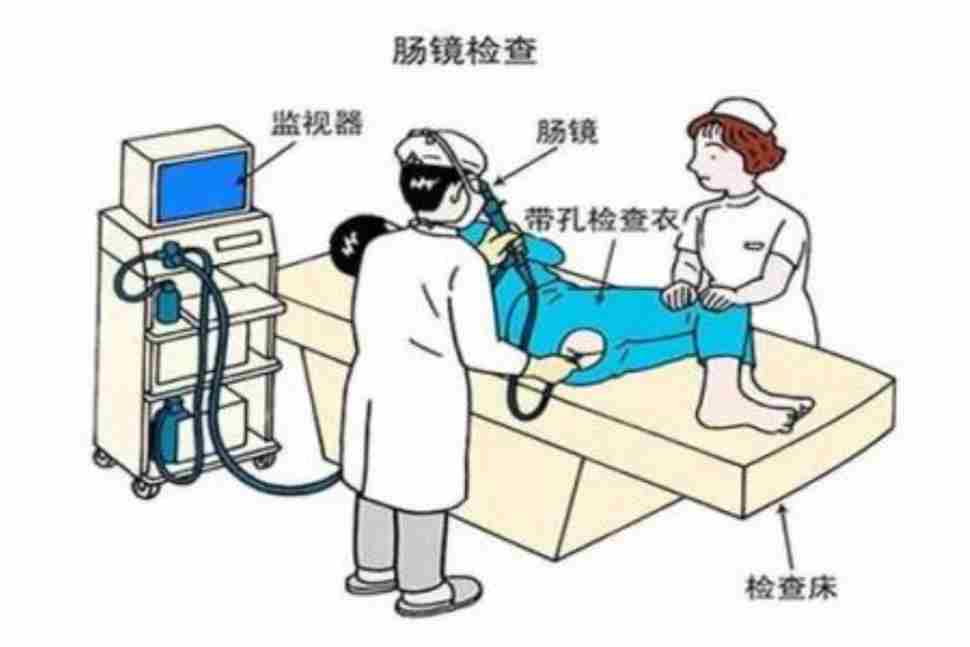
By Frieda Wiley
如果结肠癌检查不是你的首要任务,那么你并不孤单。
事实上,只有大约50%的人听从医生的指示去做结肠镜检查。但不接受检测可能会造成致命的后果。根据美国癌症协会的数据,结直肠癌在癌症相关死亡中仅次于肺癌和支气管癌,每年夺去约5万人的生命。但专家表示:好消息是,大多数结肠癌病例都可以通过筛查和养成健康的生活习惯来预防。
USPSTF的建议
美国预防服务工作组(U.S. Preventive Services Task Force)建议年龄在50至75岁之间、没有结直肠癌(CRC)风险因素的成年人每10年进行一次结肠镜检查,以筛查这种疾病。那么,如果大多数结肠癌是可以预防的,或者至少是可以治疗的,为什么那么多人不做结肠镜检查呢?也许是因为它“需要肠道准备,大多数人可能会告诉你,准备工作比实际的程序更糟糕,”Dr. Nicholas J. Petrelli是Christiana Care Health System的Helen F. Graham癌症中心和研究所的医学主任。
准备结肠镜检查
手术前一天,你可能需要采取一个明确的液体饮食和采取一系列特殊的泻药完全清空你的肠道。“另一件事是,人们需要在结肠镜检查前服用镇静剂,他们需要一个司机,还需要离开工作。”Eduardo Vilar-Sanchez, MD安德森癌症中心临床癌症预防助理教授。因此,某些人可能宁愿不做结肠镜检查,也不想影响他正常的计划!
哪怎么办?下面是另外六种筛查结肠癌的方法;其中一半是放射学检查,而其他的则是从你的粪便中提取样本。
放射学检查:电脑断层结肠镜检查或虚拟结肠镜检查
在这个过程中,技术人员将一根小管子插入直肠的前2英寸,并将空气泵入结肠,以便更好地观察。结肠的图像是用CT扫描仪在体外捕捉到的,所以你不必睡觉。
缺点:你仍然需要提前清空你的整个结肠,如果医生发现息肉或其他异常,你需要传统的结肠镜检查来仔细检查,并对任何异常组织进行活检或移除。你还需要每五年重新检查一次。
放射学检查:软性乙状结肠镜检查
与传统结肠镜检查或CT结肠镜检查不同,你不需要泻药,也不需要在检查前服用镇静剂。由于手术只检查结肠的左侧,医生可能会让你用灌肠剂清理结肠下部和直肠。
缺点:你必须每五年重新检查一次,你的医生不能检查你结肠的右侧。佩里说:“如果你的左侧有任何可能提示患病风险的检查结果,你就必须进行完整的结肠镜检查。”
放射学检查:双钡对比灌肠
也称为下消化道检查,这是最古老的CRC筛查测试之一。在使用含有咖啡基染料的灌肠剂后,结肠和直肠的异常在x光片中更容易看到。
缺点:你的医生可能会在检查前一天让你吃非乳制品的液体食物。准备好多喝一些额外的液体,按照医生的嘱咐使用泻药或灌肠剂。你需要每五年做一次检查。
粪便检测:愈创木酚粪潜血检测,简称FOBT
这种基于家庭的测试通过与红细胞中一种叫做血红素的铁结合蛋白相互作用来检测粪便中的血液。(Guaiac是一种植物物质,被用来覆盖测试卡)你不必服用镇静剂、泻药或请假。
缺点:你必须从三种不同的肠道运动中收集样本,然后把样本涂在一张卡片上,邮寄给医生进行评估。因为这个测试也能检测到血液,并给出假阳性结果,你的医生可能会让你在检查前避免食用某些食物。而且,你可能每年都要做这个测试。
基于粪便的检测:免疫化学检测或免疫组织化学检测(FIT)
是另一种类型的FOBT, FIT不需要泻药、灌肠、镇静剂或假期。然而,与愈创木鳖不同的是,你只需要收集一个样本,就可以事先吃任何你想吃的东西。
缺点:某些药物引起的轻微胃出血可能导致假阳性结果。但是根据梅奥诊所(Mayo Clinic)的胃肠病学家Dr.约翰. 基塞尔(John B. Kisiel)说,这种情况并不多见。他说:“假阳性率只有4%到6%,但如果你的筛查测试呈阳性,那么你就需要进行结肠镜检查。”
Stool-based DNA测试
这项于2014年获得美国食品和药物管理局(FDA)批准的家用检测方法,可以检测癌前、癌前或其他异常的DNA突变。不需要泻药或灌肠。使用者坐在马桶上收集粪便样本,然后准备、保存并邮寄分析。维拉-桑切斯说,这项检测比FIT和FOBT更敏感,但有两个主要缺点:“阳性检测必须通过结肠镜检查来确认。阴性测试必须重复进行,但因为测试是新的,我们还不知道应该多久进行一次。”
一切都取决于选择。
尽管专家们普遍认为,这些替代测试中没有一项特别优于其他测试,但给人们提供选择使他们更有可能接受测试。Kisiel说:“当我们给病人一个选择的时候,整体的筛查是更高的。”“当给病人提供多种测试选择时,他们更有可能接受筛查。”
If getting tested for colon cancer doesn’t top your to-do list, you’re not alone.
In fact, only about 50 percent of people follow their doctor’s orders to get a colonoscopy. But not getting tested can have deadly consequences. According to the American Cancer Society, colorectal cancer is second only to lung and bronchial cancers in cancer-related deaths, claiming about 50,000 lives each year. But the good news, experts say, is that most cases of colon cancer can be prevented through screening and adopting healthy lifestyle habits.
USPSTF recommendations
The U.S. Preventive Services Task Force recommends adults 50 to 75 years old with no risk factors for CRC have a colonoscopy once every 10 years to screen for the disease. So, if most colon cancer is preventable or at least treatable, why are so many people skipping a colonoscopy? Perhaps because it “requires bowel preparation, and most people will probably tell you that preparation is worse than the actual procedure,” says Dr. Nicholas J. Petrelli, medical director at Christiana Care Health System’s Helen F. Graham Cancer Center and Research Institute.
Prepping for a colonoscopy
The day before the procedure, you may have to adopt a clear liquid diet and take a series of special laxatives to completely empty out your bowel. “The other thing is that people have to be sedated for the colonoscopy, they need a driver and need to take off work,” says Dr. Eduardo Vilar-Sanchez, assistant professor of clinical cancer prevention at MD Anderson Cancer Center. Rather skip the colonoscopy? Here are six other ways to screen for colon cancer; half are radiological exams, while the others use samples from your stool.
Radiological exam: computed tomography colonoscopy or virtual colonoscopy
In this procedure, a technician inserts a small tube into the first 2 inches of the rectum and pumps air into the colon for better visualization. Images of the colon are captured outside the body using a CT scanner, so you don’t have to be put to sleep.
Drawbacks: You still have to empty out your entire colon beforehand, and if the doctor finds a polyp or another abnormality, you’ll need a traditional colonoscopy to take a closer look and have any abnormal tissue biopsied or removed. You also need to be retested every five years.
Radiological exam: flexible sigmoidoscopy
Unlike a traditional colonoscopy or CT colonoscopy, you won’t need laxatives or to be sedated before this test. Since the procedure only looks at the left side of the colon, your doctor will likely have you use an enema to clean out the lower part of the colon and the rectum.
Drawbacks: You must retest every five years, and your doctor can’t check the right side of your colon. “If you have any findings on the left side that may be indicative of risk, you’ll have to follow up with full colonoscopy,” Petrelli says.
Radiological exam: double-barium contrast enema
Also called a lower gastrointestinal exam, this is one of the oldest CRC screening tests. Abnormalities in the colon and rectum become easier to see in an X-ray after you use an enema containing a barium-based dye.
Drawbacks: Your doctor will likely put you on a non-dairy, liquid diet the day before the test. Be prepared to drink a lot of extra liquid and use laxatives or an enema per your doctor’s orders. You’ll need to get the test every five years.
Stool-based test: guaiac fecal occult blood test, or FOBT
This home-based test detects blood in your stool by interacting with an iron-binding protein found in red blood cells called heme. (Guaiac, a plant substance, is used to coat the test cards.) You don’t have to be sedated, take laxatives or take off work.
Drawbacks: You have to collect samples from three different bowel movements, which you smear on a card and mail in for evaluation. Because this test also detects blood found and gives false positives, your doctor will probably have you avoid certain foods before you get the exam. And, you may have to get this test every year.
Stool-based test: immunochemical test or immunohistochemical test (FIT)
Another type of FOBT, the FIT doesn’t require laxatives, enemas, sedation or vacation time. However, unlike the guaiac FOBT, you only need to collect one sample and can eat whatever you want beforehand.
Drawbacks: Minor stomach bleeding caused by certain medications can give false positives results. But according to Dr. John B. Kisiel, a gastroenterologist at the Mayo Clinic, those instances are low. “The false positive rate is only about 4 to 6 percent, but if you have a positive screening test, then you’ll need a diagnostic colonoscopy,” he says.
Stool-based DNA test
Approved by the Food and Drug Administration in 2014, this at-home test checks for DNA mutations that are precancerous, cancerous or otherwise abnormal. No laxatives or enemas are required. Users collect a stool sample while sitting on the toilet, which they then prepare, preserve and mail in for analysis. Vilar-Sanchez says the test is more sensitive than FIT and FOBT but has two major drawbacks: “A positive test must be confirmed with colonoscopy. Negative tests must be repeated, but because the test is new, we don’t know how often that should be yet.”
It’s all about options.
While experts generally agree none of these alternative tests are particularly better than another, giving people options makes them more likely to get tested. “When we give patients a choice, the overall screening is higher,” Kisiel says. “Patients are more likely to get screened when they are offered a choice of tests.”


{kind=link}
{kind=link}
{kind=link}