- 如有疑问,请联系电邮
- customer@ihealth66.com


USNEWS:是肺癌还是别的什么?先不要紧张!

USNEWS:肺癌是如何扩散的
2019年3月26日
USNEWS:需要了解年轻患者的肺癌原因
2019年3月28日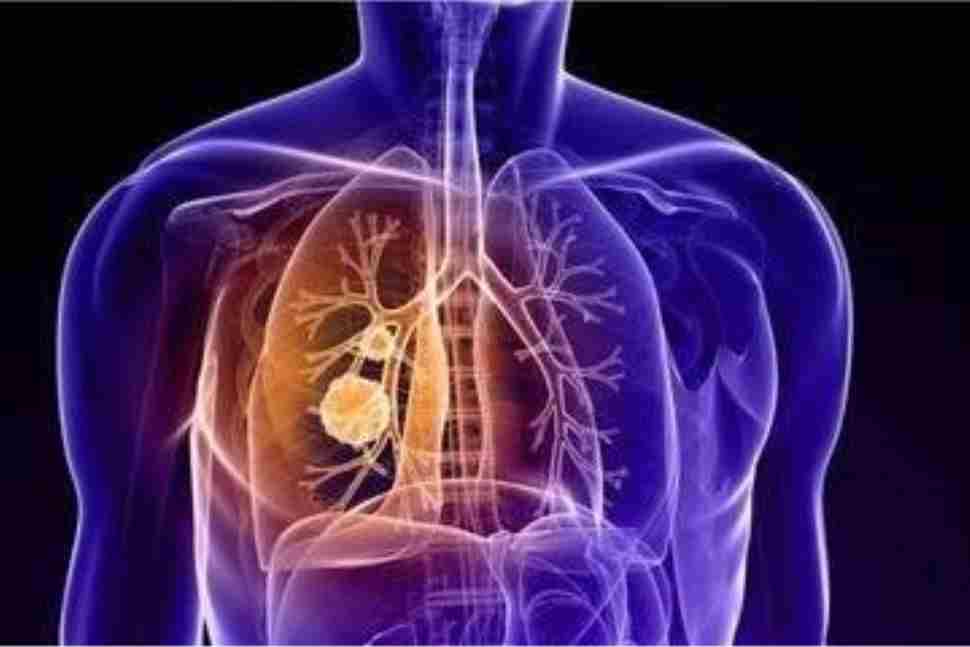
By Kathleen Hall
听到在肺部扫描或胸部x光检查中有异常是很可怕的,可能首先想到的是得了癌症。虽然这可能是真的,但更有可能的是,令人担忧的发现并没有那么严重。事实上,发现结节或小肿块是很常见的。它在医学成像扫描中以阴影或斑点的形式出现。
根据美国胸科学会的说法,这些结节有几个可能的原因,包括你可能没有意识到的旧感染留下的疤痕组织,或者是环境中的某种刺激。ATS说,在接受胸部x光或CT扫描的成年人中,多达一半的人有结节;其中大部分都很小,不会引起疼痛或呼吸问题。
仔细想想,这是有道理的。纽约纪念斯隆-凯特琳癌症中心(Memorial Sloan-Kettering Cancer Center)的肺科医生马克·范斯坦(Marc Feinstein)说:“婴儿天生拥有完美的皮肤。”“随着年龄的增长,他们会有疤痕、老年斑和雀斑。然而,其中很少是黑色素瘤(一种皮肤癌)。”肺也是一样。幸运的是,尽管这些异常可能在影像学检查中模拟肺癌,但大多数并不是真正的肺癌。
那么,你怎么知道是不是肺癌呢?
佛罗里达大学健康癌症中心-奥兰多健康罗德·泰勒胸科护理中心的医学主任路易斯·埃雷拉博士说,有三种方法可以让你知道自己患有肺癌:
- 你有症状,去看医生,医生在CT扫描或x光片上发现可疑肿块。然而,Herrera说,85%的肺癌患者从未出现症状。此外,肺癌的症状,如持续咳嗽、背痛或体重减轻,可能类似感冒或支气管炎,但可能不会引起肺癌的怀疑。然而,Herrera说,如果你有这样的症状,几周内不会消失,那就去看医生。
- 你接受胸部x光检查的原因与此无关(例如,在手术前),这表明你的肺部有一个斑点。
- 因为你是个烟鬼,你参加了肺癌筛查。
确切地说,肺癌是如何被发现的是相关的,因为对肺癌高危人群实施筛查意味着更多的人在他们的肺部发现了一些东西。通常情况下,这一发现是假阳性:扫描结果似乎不正常,尽管这个人实际上并没有癌症。
在全国肺筛查试验中,近5.4万名年龄在55岁至74岁之间、有严重吸烟史(吸烟被认为是罹患肺癌的高风险)的人接受了标准胸透或低剂量螺旋ct筛查。试验显示,CT扫描在发现早期肺癌方面比x光更好。接受低剂量CT扫描的参与者死于肺癌的风险比接受标准胸透的参与者低15%到20%(自试验以来,肺癌死亡率的降低已更新为16%)。
然而,筛查的假阳性率接近25%。这意味着大约四分之一的人在经过三轮筛查后会发现异常。其中96%的人不会得肺癌。
范斯坦说,关键是要区分良性结节和恶性结节。肿瘤学家必须确定一个异常的发现是否可能实际上表明肺癌,并需要进一步的分析。如果一个人是重度吸烟者,那么这种异常比不吸烟者更令人担忧。范斯坦说,医生也会观察斑点的特征。他说:“如果肿瘤非常大(10厘米或更大),就更有可能是癌症。”“如果边界不规则,就更有可能患上癌症。”
如果这种异常没有立即提示肺癌的特征,医生可以做后续扫描,看看结节是否随着时间的推移而改变,例如:生长。ATS说大多数肺癌生长缓慢,所以在做额外的检查前等待下一次CT扫描通常是可以的。此外,对一个小结节做活检可能会导致副作用,如肺部塌陷或感染。
肺癌筛查的高假阳性率令一些卫生专业人士感到担忧。在《美国医学会内科杂志》(JAMA Internal Medicine)的一篇社论中,几名医生指出,假阳性可能导致额外的、潜在的侵入性和高风险的诊断程序以确定是否存在癌症。作者写道:“每1000名接受筛查的人中,就有10人被诊断为早期肺癌(可能治愈),5人被诊断为晚期肺癌(无法治愈);20例将接受与筛查直接相关的不必要的侵入性手术;550人将经历不必要的警报和反复的CT扫描(这与辐射有关)。”
谁应该接受肺癌筛查?
美国预防服务工作组和美国胸科学会推荐,在55到80岁的成年人有30 pack-year吸烟史(“包年”意味着你每天抽一盒,有30年或等效历史),目前吸烟或戒烟在过去15年,接受年度低剂量CT筛查肺癌。如果你有大量吸烟的历史,和你的医生谈谈肺癌筛查的利弊。当然,早期发现肺癌的预后最好,Herrera说,在这种情况下,你应该咨询肺癌专家,以确保你得到了正确的评估和治疗。
HEARING THAT YOU HAVE something abnormal on a lung scan or chest X-rayis scary. The first thing you probably assume is that you have cancer. While that may be true, it’s far more likely that the worrisome finding is something less serious. It’s actually very common to find a nodule, or small mass. It appears as a shadow or spot on a medical imaging scan.
According to the American Thoracic Society, these nodules have several likely causes, including scar tissue from an old infection you might not have realized you had or an irritation from something in the environment. The ATS says up to one half of adults who get a chest X-ray or CT scan have a nodule; most of these are very small and don’t cause pain or breathing problems.
It makes sense, when you think about it. “A baby is born with perfect skin,” says Dr. Marc Feinstein, a pulmonologist at Memorial Sloan-Kettering Cancer Center in New York. “As a person ages, they get scars, age spots, freckles. Few of these are melanoma [a form of skin cancer], however.” It’s the same way with the lungs. Fortunately, although these abnormalities might mimic lung cancer on an imaging test, most are not actually lung cancer.
So, How Do You Know if It’s Lung Cancer?
There are three ways you can learn you have lung cancer, says Dr. Luis Herrera, medical director of the Rod Taylor Thoracic Care Center at UF Health Cancer Center – Orlando Health:
- You have symptoms and see your doctor, who then finds a suspicious mass on a CT scan or X-ray. However, Herrera says, 85 percent of people with lung cancer never have symptoms. Furthermore, lung cancer symptoms, such as a persistent cough, back pain or weight loss, can resemble a cold or bronchitis and may not raise suspicions of lung cancer. However, Herrera says, if you have symptoms like these that don’t go away in a few weeks, seek medical attention.
- You undergo a chest X-ray for an unrelated reason (for example, before surgery), which indicates a spot in your lung.
- Because you were a heavy smoker, you participate in lung cancer screening.
Exactly how lung cancer is discovered is relevant because implementing screening for people at high risk of lung cancer means more people are finding something on their lungs. Often, the finding is a false positive: The scan appears abnormal, although the individual doesn’t actually have cancer.
In the National Lung Screening Trial, nearly 54,000 people ages 55 to 74 with a history of heavy smoking (which is considered a high risk for developing lung cancer) were screened either with a standard chest X-ray or with low-dose helical computed tomography. The trial revealed that CT scans were better than X-rays at finding early stage lung cancers. Participants who received low-dose CT scans had a 15 to 20 percent lower risk of dying from lung cancer than participants who received standard chest X-rays (since the trial, this reduction in lung cancer mortality has been updated to 16 percent).
However, the false positive rate from screening is nearly 25 percent. That means approximately 1 in 4 people who are screened over three rounds of screening exams will have an abnormal finding. Of those, 96 percent will not have lung cancer.
Feinstein says the trick is to distinguish benign nodules from malignant ones. Oncologists must determine if an abnormal finding may in fact indicate lung cancer and warrant further analysis. If the individual is a heavy smoker, an abnormality is more worrisome than one in a non-smoker. Feinstein says doctors also look at the characteristics of the spots. “If it’s very big [10 centimeters or larger], it’s more likely to be cancer,” he says. “If it has irregular borders, it’s more likely cancer.”
If the abnormality does not have characteristics that immediately suggest lung cancer, physicians can do follow- up scans to see if the nodule changes – for example, grows – over time. The ATS says most lung cancers grow slowly, so it’s usually OK to wait for the next CT scan before doing additional tests. Plus, doing a biopsy on a small nodule could cause adverse effects, such as a collapsed lung or infection.
The high rate of false positives in lung cancer screening is concerning to some health professionals. In an editorial in JAMA Internal Medicine, several doctors made the point that false positives can lead to additional, potentially invasive and risky diagnostic procedures to determine if cancer is present. The authors wrote: “For every 1,000 people screened, 10 will be diagnosed with early-stage lung cancer (potentially curable), and five with advanced-stage lung cancer (incurable); 20 will undergo unnecessary invasive procedures directly related to the screening; and 550 will experience unnecessary alarm and repeated CT scanning, [which is associated with radiation].”
Who Should Be Screened for Lung Cancer?
The U.S. Preventive Services Task Force and American Thoracic Society recommend annual screening for lung cancer with low-dose computed tomography in adults 55 to 80 who have a 30 pack-year smoking history (a pack year means you smoked one pack per day for 30 years or the equivalent) and currently smoke or quit within the past 15 years. If you have a history of heavy smoking, talk to your doctor about the pros and cons of lung cancer screening. Of course, the prognosis for lung cancer is best when you detect it early, Herrera says, in which case, you should consult with a lung cancer expert to ensure you’re properly evaluated and treated.


{kind=link}
{kind=link}
{kind=link}