- 如有疑问,请联系电邮
- customer@ihealth66.com


USNEWS:结肠癌的早期征兆

USNEWS:7种预防皮肤癌的方法
2019年3月20日
USNEWS:2020肺癌患者指南
2019年3月22日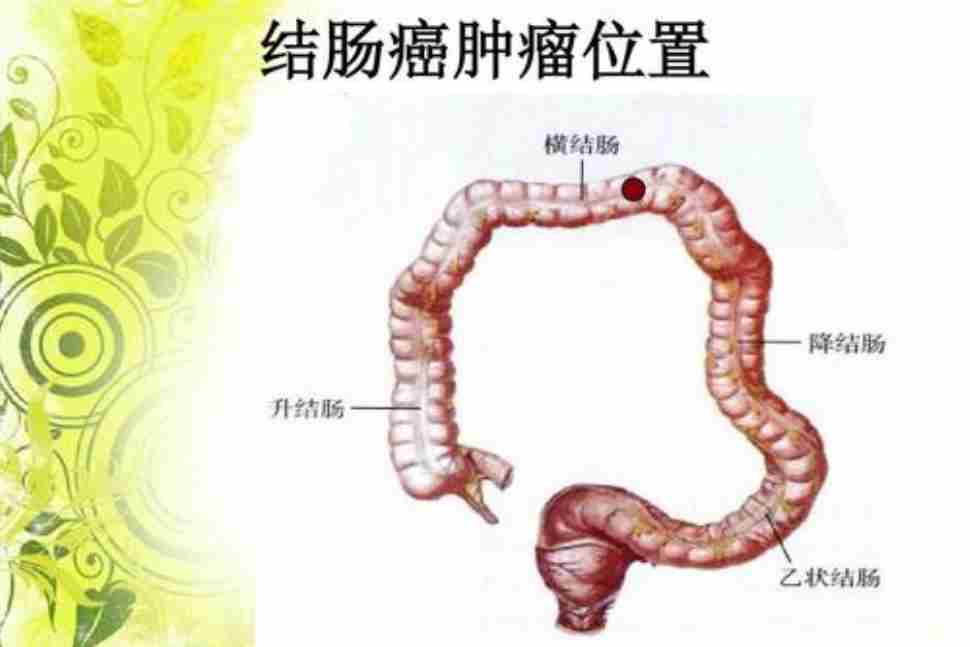
By Elaine K. Howley
回想起来,有一些模糊的迹象表明出了什么问题。现年45岁的里克·奥斯特伯格(Rick Osterberg)就是这么说的。他在接受了长达一年的结肠癌第三阶段积极治疗后,于2018年12月被宣布无癌。2017年夏天,大约在确诊前6个月,他在伦敦度假时与便秘作斗争。“当我们回到家的时候,问题基本上解决了,所以我把原因归结于旅行和不熟悉的食物。”
然后,在2017年9月,癌症确诊前大约三个月,他出现了更轻微的便秘和胃肠痉挛。把他送去看医生已经够糟糕的了,但考虑到他“几十年来偶尔会感到胃部敏感”,这种不适被归因为轻度肠易激综合征。奥斯特伯格被建议服用纤维补充剂,这足以帮助“我认为它解决了。”
但在2017年12月,奥斯特伯格说他出现了低烧——99.5华氏度——“感觉有点不舒服。”
医生做了血检,没有发现危险信号。“他建议,如果几周内情况没有好转,我就回来。他们没有好转,所以两周后我回来了,症状没有改变。他说,额外的血检没有显示出任何令人担忧的迹象。尽管对单核细胞增多症的检测呈阴性,但医生仍怀疑这是一种持续性病毒感染。单核细胞增多症是一种常见的病毒感染,会导致低烧和疲劳。但他还有另一种本能,那就是排除更大的可能性。他说他要做一个CT扫描,这样我们就可以排除一大堆‘可怕的东西’,只要能让我对‘可怕的东西’不那么担心,”奥斯特伯格回忆道。
当时的CT扫描结果很可怕。医生告诉奥斯特伯格,他的乙状结肠有一个肿块,乙状结肠是大肠中最靠近直肠和肛门的部分。他立即被安排接受结肠镜检查——这是一种医生将摄像机插入结肠以观察里面有什么东西的过程。癌细胞开始扩散,因此奥斯特伯格被诊断为结肠癌第三阶段,这是一种严重但可以治疗的疾病。
结肠癌是如何开始的?
结肠癌,有时也被称为结肠直肠癌,通常开始时是一种非癌性生长,称为结肠内壁息肉,也被称为大肠,是消化道的主要组成部分。结肠和直肠一起形成大肠,大肠是一根长管,从大部分被消化的食物中提取营养物质,并将废物转移到肛门进行排泄。
奥兰多佛罗里达大学健康癌症中心(Orlando Health UF Health Cancer Center)肝脏和胰腺中心(Liver Center and胰腺Center)的医学肿瘤学家/血液学家斯瑞拉姆·马迪帕特拉(Sreeram Maddipatla)博士说,息肉会随着时间的推移自然发生。“这些是在结肠内壁形成的一小块细胞。大多数结肠息肉是无害的,但其中一些可能发展成癌症。“增生性息肉是良性的,通常不会造成威胁,但通常会被切除,因为它们会生长并造成阻塞。”但另一种类型的息肉,称为腺瘤或腺瘤性息肉,可能会癌变,需要切除。
息肉的形成有多种原因,与遗传、纤维摄入不足、饮食中红肉含量高等因素有关。“随着时间的推移,某些突变会发生在结肠内壁,形成息肉。息肉需要5到10年的时间才能转变成癌症。息肉在老年人中更为常见,当它们癌变时,可能会致命。
纽约纪念斯隆凯特琳癌症中心(Memorial Sloan Kettering cancer Center)的结直肠外科医生埃马努伊p帕普(Emmanouil P. Pappou)说,结肠癌是男性和女性第三大最常见的癌症。他说:“在美国,大约每20个人中就有1人受到这种疾病的影响。我们每年大约有14.5万大肠癌病例,大约5万人死于大肠癌,大约占所有癌症死亡人数的8%,所以这是一个重要的问题。”
过去,结直肠癌最常在老年人中发现,但帕普说:“在过去几十年里,年轻人中结直肠癌的发病率有所上升。在确诊时,奥斯特伯格只有44岁,还是一名游泳健将,是这些年轻人中的一员。他不符合结肠癌患者的典型特征,因为这种疾病往往在饮食不健康、超重或肥胖、缺乏锻炼的老年人中更为常见。
但奥斯特伯格缺乏这种疾病的警告信号和特定症状的经验是相当普遍的。许多被诊断出结肠癌的人没有任何症状,这也是为什么这种疾病通常在晚期才被诊断出来的原因之一。
马迪帕特拉说:“很多时候,你可能根本没有症状,如果你有症状,最常见的就是排便习惯的改变或大便稠度的变化,这种变化会持续几周以上。”正如奥斯特伯格所经历的,这些症状很容易被忽视,因为吃了一些不寻常的东西或消化不良的结果。大多数人不会马上把便秘和结肠癌联系起来。
帕普列举了结直肠癌的早期症状如下:
- 便秘
- 排便习惯的改变
- 腹泻
- 便血
- 大便的宽度变窄或改变
- 不完全疏散的感觉
- 抽筋的痛苦
- 疲劳
- 原因不明的体重减轻
问题是,当症状被忽视或被错误地归因于另一种疾病时,比如病毒感染或肠易激综合征,会给癌症更多的生长时间,在被发现之前,癌症可能会发展到晚期。美国癌症协会(American Cancer Society)报告称,“只有39%的CRC患者被诊断出患有局部期疾病(尚未扩散到附近组织的最早阶段),五年生存率为90%;被诊断为局部和远处癌症的患者存活率分别下降到71%和14%。”
很明显,早期诊断结肠癌有助于生存,但在早期阶段几乎没有明显的症状,这是一个具有挑战性的命题。输入筛选。
为什么结肠癌筛查很重要?
美国癌症协会(American Cancer Society)建议,从45岁开始定期进行结直肠癌筛查。帕普说,美国癌症协会最近将结直肠癌筛查的年龄从50岁下调,以帮助解决年轻人被诊断出结直肠癌的问题。美国癌症协会表示,如果你身体健康,预期寿命超过10年,那么在75岁之前,成年人应该继续进行常规筛查。对于75岁至85岁的人,你的医生可以建议你继续筛查是否有意义。85岁以上的人不建议继续定期接受结直肠癌筛查。
这些筛查测试可以作为一种基于粪便的测试来进行,以寻找一个人粪便中的癌症迹象,也可以通过结肠镜或乙状结肠镜来进行——这两种视觉测试都是将摄像机插入结肠以寻找息肉。帕普称结肠镜检查是“筛查的黄金标准”,并将其描述为“当日门诊程序”。“人们必须接受肠道准备,”这意味着喝一种强有力的泻药溶液来清洁肠道,这样医生就能看到结肠的内壁。这种制剂“通常耐受性很好,但它通常是制剂中最麻烦的部分”。“检查结果的质量取决于医生对结肠的观察程度,因此,无论检查结果有多令人不快,在准备结肠镜检查时,一定要遵循医嘱,这一点很重要。”
我能预防结肠癌吗?
帕普说:“结肠镜检查的神奇之处在于,它是我们在21世纪拥有的唯一一种可以预防癌症的检查方法。”“我们拥有的所有其他筛查工具——乳房x光检查、宫颈巴氏涂片检查和超声波——都擅长早期发现癌症。但他们无法阻止。这是我们所知道的唯一可以预防形成的癌症,因为如果(医生)发现息肉,他们可以在它们变成癌症之前将其切除。帕普说,流行病学研究已经证实了这一点。“摘除息肉的人得癌症的几率要小得多。它的工作原理。”
他说,息肉癌变可能需要10年时间,因此结肠癌通常需要很长时间才能发展。这就是为什么筛查,尤其是在更年轻的时候,可能特别有用。“我在35岁的时候做了这个手术,这是我个人的建议。这是预防测试。我们确实说过一盎司的预防要比一磅的治疗更有价值,”所以他建议,如果可能的话,尽早开始结肠直肠癌筛查。
Maddipatla表示同意。“我告诉我的病人尽早接受筛查。“特别是,有癌症、结肠癌、息肉或结肠癌家族史的人应该定期接受筛查。
对于所有的病人,Maddipatla说,“我也告诉他们遵循健康的饮食,包括水果,蔬菜和全谷物。此外,要有足够的锻炼并保持体重,“因为肥胖或超重会增加患结肠癌的风险。”
此外,他说:“一些研究表明,每天服用婴儿阿司匹林可能会有帮助。一些研究表明,长期服用低剂量阿司匹林可将结直肠癌前息肉的发病率降低50%。阿司匹林可以减少体内的炎症,从而降低基因突变发生并导致癌症的几率。和你的初级保健医生谈谈每天服用阿司匹林是否适合你的情况。
帕普补充说,避免某些食物和行为也可以降低患结肠癌的风险。具体来说,避免:
- 吸烟
- 过量饮酒
- 吃过多的红肉
- 摄入过多的卡路里
- 喝含糖和碳酸饮料
虽然筛查和选择健康的生活方式可能有所帮助,但结直肠癌仍有遗传因素,”但这并不是所有人的答案。很多病例都与运动和饮食有关。
尽管如此,他说:“我们不可能永远存在,一些机制很容易崩溃。“结肠是身体的一部分,可能会受到年龄的影响。但他说:“预防癌症最重要的是定期锻炼身体。每天只需30分钟的步行或一些低能量的运动,比如室内自行车,“就能产生效果。”帕普说,你不必成为马拉松运动员或健身傻瓜,只要把更多的运动融入日常生活就足够了。
说出来
奥斯特伯格说,他很感激他和他的初级保健医生有关系。“我真的不知道是什么原因让我的PCP认为我们应该做CT扫描来排除一些因素,但至少有一些可能是基于我们现有的关系,”他说。“他做我的PCP大概有20年了,我可能在传达一些东西——也许是我自己的直觉(请原谅我的双关语)暗示了某种东西不仅仅是一种冬季病毒,这让他有了一种本能”去做额外的测试。
这种本能很可能救了奥斯特伯格的命。“例如,如果我带着完全相同的症状去了一家急诊诊所,我可能会被更多地诊断为‘这只是一种持续性病毒’。几个月后,我可能会因为肿瘤引起的肠梗阻而出现在急诊科,情况可能会更糟。”
LOOKING BACK, THERE were a few vague signs that something was wrong. So says Rick Osterberg, 45, who was declared cancer-free in December 2018 after a long year of aggressive treatment for stage 3 colon cancer. In the summer of 2017, about six months before he was diagnosed, he struggled with constipation while on vacation in London. “It largely resolved when we got home, so I attributed it to travel and unfamiliar food.”
Then, in September 2017, about three months prior to the cancer diagnosis, he had more mild constipation and gastrointestinal cramping. It was bad enough to send him to the doctor, but given that he’d had an “occasionally sensitive stomach for decades,” the discomfort was chalked up to a mild case of irritable bowel syndrome. Osterberg was advised to take fiber supplements, which helped enough that “I considered it resolved.”
But then in December 2017, Osterberg says he developed a low-grade fever – 99.5 degrees Fahrenheit – “and was feeling a bit off.” He went to the doctor and was told, “quite reasonably,” that it was “likely a seasonal virus of some kind that I was fighting off.”
The doctor did bloodwork, which turned up no red flags. “He advised that I come back if things didn’t improve in a couple weeks. They didn’t improve, so I was back two weeks later with symptoms unchanged.” Additional bloodwork showed nothing alarming, he says. Although a test for mononucleosis, a common viral infection that causes low-grade fever and fatigue, came back negative, the doctor still suspected a persistent viral infection. “But he had another instinct that said to rule out bigger things. He said that he was going to order a CT scan so that we could rule out a whole bunch of ‘scary stuff’ if only so that it would make me less anxious about ‘scary stuff,’” Osterberg recalls.
That CT scan, as it happened, turned up something scary. The doctor told Osterberg there was a mass in his sigmoid colon, the part of the large intestine closest to the rectum and anus. He was immediately scheduled for a colonoscopy – a procedure in which a doctor threads a camera into the colon to have a look at what’s inside. The growth was cancerous and had begun to spread, so Osterberg was diagnosed with stage 3 colon cancer, a serious but treatable disease.
How Does Colon Cancer Start?
Colon cancer, also sometimes called colorectal cancer, usually starts out as a noncancerous growth called a polyp inside the inner lining of the colon, also known as the large intestine and a major component of the digestive tract. Together, the colon and the rectum form the large intestine, a long tube that extracts nutrients from mostly digested food and moves waste products to the anus for excretion.
Dr. Sreeram Maddipatla, a medical oncologist/hematologist for the Liver Center and Pancreas Center at Orlando Health UF Health Cancer Center, says polyps naturally occur over time. “These are a small lump of cells that forms on the lining of the colon. Most colon polyps are harmless, but some of them may develop into cancer.” Hyperplastic polyps are benign and don’t usually pose a threat, but are often removed because they can grow and cause obstructions. But another type of polyp, called adenomas or adenomatous polyps, can turn cancerous and need to be removed.
Polyps form for a variety of reasons related to genetics, not eating enough fiber, eating a diet high in red meat and other risk factors. “Over time, certain mutations will happen in the lining of the colon that will form these polyps. It takes five or 10 years for polyps to turn into cancer,” Maddipatla says. Polyps are more common in older adults and when they turn cancerous, they can become deadly.
“Colon cancer is the third most commonly diagnosed cancer in both men and women, says Dr. Emmanouil P. Pappou, a colorectal surgeon at Memorial Sloan Kettering Cancer Center in New York. “It affects roughly about 1 out of 20 people in the United States. We have about 145,000 cases of large intestinal cancer every year and about 50,000 people succumb to this cancer, accounting for roughly 8 percent of all cancer deaths, so it’s a significant issue,” he says.
In the past, colorectal cancer was most often found in older adults, but Pappou says that “over the past few decades, there’s been a rise in this cancer among younger people.” At just 44 years old at the time of diagnosis and a competitive swimmer, Osterberg was one of these younger people. He didn’t fit the typical profile for colon cancer patient, as the disease tends to be more common among older adults who don’t eat healthfully, are overweight or obese and don’t exercise enough.
But Osterberg’s experience regarding a lack of warning signs and specific symptoms of the disease is quite common. Many people diagnosed with colon cancer experience no symptoms, and this is one reason why the disease is often diagnosed in later stages.
“A lot of times you may not have symptoms at all, and if you have them, the most common ones are changes in bowel habits or changes in the consistency of your stool that lasts for more than a few weeks,” Maddipatla says. Such symptoms, as Osterberg experienced, are easily overlooked as being the result of eating something unusual or a bit of indigestion. Most people wouldn’t make the leap to connect a bit of constipation to colon cancer right away.
Pappou lists early signs of colorectal cancer as being:
- Constipation
- Changes in bowel habits
- Diarrhea
- Blood in stool
- A narrowing or change in girth of the stool
- A feeling of incomplete evacuation
- Cramping pains
- Fatigue
- Unexplained weight loss
The problem is that when symptoms are overlooked or incorrectly ascribed to another condition, such as a viral infection or irritable bowel syndrome, that affords the cancer more time to grow, and it can progress to later stages before being detected. The American Cancer Society reports that “only 39 percent of CRC patients are diagnosed with localized-stage disease (the earliest stage that has not spread to nearby tissues) for which the five-year survival rate is 90 percent; survival declines to 71 percent and 14 percent for patients diagnosed with regional and distant stages respectively.”
It’s clear that diagnosing colon cancer early aids in survival, but with so few symptoms noticeable in the early stages, this is a challenging proposition. Enter screening.
Why Is Screening for Colon Cancer Important?
The American Cancer Society recommends starting regular colorectal cancer screening at age 45, a recommendation that Pappou says the ACS recently lowered from age 50 to help address the rise in younger people being diagnosed with this form of cancer. The ACS says adults should continue routine screening through age of 75 if you’re in good health with a life expectancy of more than 10 years. For people aged 75 to 85, your doctor can advise you as to whether continued screening makes sense. People over age 85 are not recommended to continue having regular colorectal cancer screening.
These screening tests can be conducted as a stool-based test that looks for signs of cancer in a person’s stool, or via a colonoscopy or sigmoidoscopy – both visual tests that insert a camera into the colon to look for polyps. Pappou calls colonoscopy “the gold-standard for screening,” and describes it as a “same-day, outpatient procedure. People have to receive a bowel preparation,” which means drinking a powerful laxative solution to clean the bowels so that the doctor can see the internal lining of the colon. That preparation “is usually well tolerated, but it’s usually the most bothersome part of the preparation.” The quality of the test results is dependent on how good a look the doctor can get at the colon, so it’s important to follow orders for readying your colon for a colonoscopy, no matter how unpleasant it might be.
Can I Prevent Colon Cancer?
“The miraculous thing about colonoscopy is that it’s the only test that we have in the 21st century that can prevent you from getting cancer,” Pappou says. “All the other screening tools that we have – mammograms, cervical pap smears and ultrasounds – are good at finding cancer early. But they can’t prevent it. This is the only cancer that we know we can prevent from forming because if the (doctor) finds polyps, they can remove them before they turn into cancer.” Pappou says this has been proven via epidemiological studies. “People who get their polyps removed get far, far less cancer. It works.”
He says it can take 10 years for a polyp to turn cancerous, so colon cancer typically takes a long time to develop. This is why screening, especially at a younger age, can be particularly useful. “I had mine done at age 35, and that’s my personal recommendation. It’s a prophylactic test. We do say an ounce of prevention is worth a pound of cure,” so he recommends getting started early if you can with colorectal screening.
Maddipatla agrees. “I tell my patients to get the screening early.” In particular, people who have a personal history with cancer, colon cancer, polyps or a family history of colon cancer should be screened regularly.
For all patients, Maddipatla says, “I also tell them to follow a healthy diet, which includes fruits, vegetables and whole grains. Also, get enough exercise and maintain weight,” because being obese or overweight has been linked to a higher risk of developing colorectal cancer.
In addition, he says “there are some studies showing that taking a baby aspirin daily could be helpful.” Long-term, low-dose aspirin use has been shown to lower the rate of precancerous colorectal polyps by as much as 50 percent, according to some studies. Aspirin reduces inflammation in the body, which can reduce the chances that genetic mutations will occur that could lead to cancer. Talk to your primary care provider about whether adding a daily aspirin is right for your situation.
Pappou adds that avoiding certain foods and actions can also reduce your risk of developing colon cancer. Specifically, avoid:
- Smoking
- Drinking excessive amounts of alcohol
- Eating excessive amounts of red meat
- Consuming excessive amounts of calories
- Drinking sugary and carbonated drinks
While screening and making healthy lifestyle choices can help, there’s still a genetic component to colorectal cancer, “but it’s not the answer for everyone. A lot of cases are associated with activity and diet,” Pappou says.
Still, he says “we’re not meant to last forever and some mechanisms are prone to breaking down.” The colon is one part of the body that seems likely to suffer the consequences of age. But he says “the most important thing you can do to prevent cancer is regular physical exercise. Just 30 minutes of walking every day or something low-energy like indoor biking” can make a difference. You don’t have to become a marathon runner or a fitness fool – just incorporating more movement into your daily routine is enough to offer benefits, Pappou says.
Speak Up
Osterberg says he’s grateful he had a relationship with his primary care doctor. “I don’t really know what caused my PCP to think we ought to do a CT scan to rule some things out, but at least some of it was probably based on the existing relationship we had,” he says. “He’s been my PCP for perhaps 20 years now, and there was probably something about how I was conveying things – perhaps my own gut (pardon the pun) suggesting something was more than a winter virus that caused him to have a bit of an instinct” to run additional tests.
This instinct may well have saved Osterberg’s life. “If, for example, I had gone into an urgent care clinic with the exact same symptoms, I might have been sent away with more of a ‘it’s just a persistent virus’ sort of diagnosis. Then I might have presented in the emergency department several months later with a bowel obstruction from the tumor, and things would have been a lot worse.”


{kind=link}
{kind=link}
{kind=link}